An exchange standard such as HL7 CDA R2 fixes the structure of a clinical document but not the words used to describe a diagnosis, a test or a finding: those come from external vocabularies, and picking the wrong one is among the most common reasons a clinical datum later turns out to be impossible to reuse. SNOMED CT, LOINC and the ICD family cover three distinct jobs; confusing them produces codings that are technically valid and semantically useless.
Context
A controlled clinical terminology is a set of concepts, each with a stable identifier, formal relationships and a governance that maintains them over time. A code inside a CDA message is valid locally; it becomes comparable across systems only if it belongs to a shared, versioned vocabulary. Secondary use — multicentre research, epidemiology, planning — works on one condition: the same meaning must carry the same code across hospitals, regions and countries.
What separates the three vocabularies is not quality but the semantic axis. SNOMED CT answers “what does the patient have”. LOINC answers “what was observed or measured”. ICD answers “which statistical or reimbursement class the case falls into”. The three answers do not substitute for one another.
SNOMED CT
SNOMED CT (Systematized Nomenclature of Medicine — Clinical Terms) is the most extensive clinical terminology in production. It was formed in 2002 by merging the College of American Pathologists’ SNOMED with the NHS’s Clinical Terms Version 3; since 2007 it has belonged to SNOMED International, a not-for-profit based in the United Kingdom with national members in more than thirty countries. The International Edition ships twice a year: the January 2017 release added 5,123 concepts, including the first Lateralizable Body Structure Reference Set, together with contributions from Kaiser Permanente’s Convergent Medical Terminology and from Orphanet.
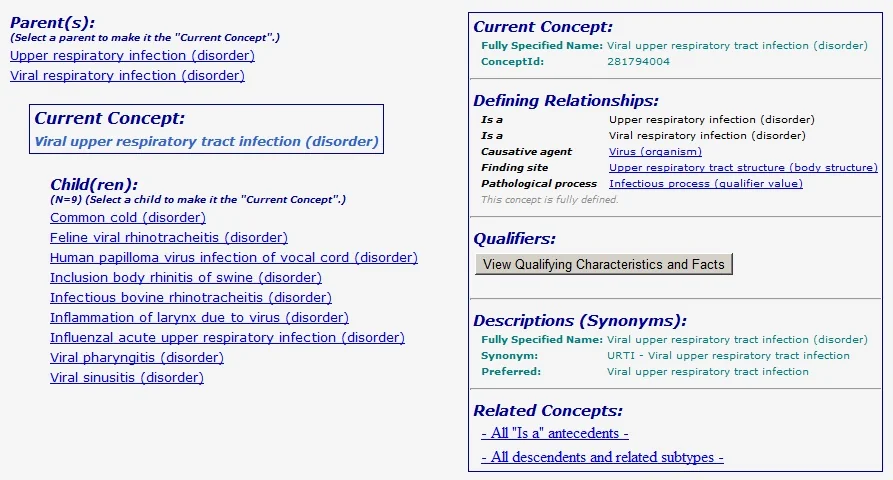
Each concept has a numeric identifier (SCTID), a Fully Specified Name and synonym descriptions. IS-A relationships form a poly-hierarchical taxonomy — a concept may have several parents — alongside domain relationships such as finding site, associated morphology and causative agent. Two features separate SNOMED CT from classifications:
- post-coordination: a meaning that is not pre-coded is composed by combining concepts that already exist (fracture of tibial shaft + due to fall);
- Reference Sets, official or national subsets that restrict the concepts admissible in a given context and keep a vocabulary of hundreds of thousands of entries in check.
Formal querying uses the Expression Constraint Language (ECL): an expression such as << 64572001 selects every subtype of the concept “disease” inside a coded record, something a flat list of codes cannot do.
Adoption runs through the state joining SNOMED International, with fees proportional to national income. Italy is not a member as of this date: SNOMED CT is used under research licences or in scoped projects. The gap relative to the United Kingdom, Scandinavia, Germany and the Netherlands comes up often in the debate around the Italian electronic health record.
LOINC
LOINC (Logical Observation Identifiers Names and Codes) names observations: laboratory tests, clinical measurements, and also document and section types. The Regenstrief Institute in Indianapolis has developed it since 1994 and distributes it free of charge, under a licence that permits use in commercial or open-source software. The current version is 2.59, of February 2017; the term count has stood above 85,000 since version 2.58 of December 2016.
A LOINC code comes out of a six-axis model: Component (what is measured), Property (physical property), Time (timing interval), System (material or context), Scale (measurement scale), Method (optional). Thus 1558-6 denotes a fasting plasma glucose in serum or plasma, by mass per volume. Once broken into these axes, the same measurement stays comparable even when laboratories call it by different names.
LOINC also supplies the document- and section-type codes used in the header and body of Italian CDA R2 documents — for instance 34133-9 for an episode summary note, 11502-2 for a laboratory report. In Italy the HL7 Italia CDA R2 profiles adopt LOINC for the laboratory and for document sections; since 2012 there has been an official Italian translation, which localises the descriptions and keeps the numeric codes of the international edition.
The critical point
The most expensive mistake is using ICD where SNOMED CT is needed, or the reverse. The ICD family (International Classification of Diseases), maintained by the World Health Organization, is a classification, not a clinical terminology: it groups cases into mutually exclusive, collectively exhaustive categories tuned for mortality and morbidity statistics and for reimbursement. ICD-10, in its WHO 2016 version, is the standard for causes of death; ICD-10-CM, the United States clinical modification, replaced ICD-9-CM for morbidity from 1 October 2015; ICD-11 is in beta draft, frozen for field testing and not yet adopted.
The difference is structural: ICD forces a choice, every case ends up in one and only one category, even when the real picture is finer than the available classes. SNOMED CT describes the case at the granularity needed and allows several concepts to coexist. If I code the record in ICD and then expect to run fine clinical analysis on it, I have already lost the information upstream; if I code in SNOMED CT and need a reimbursement statistic, a mapping is enough. The right flow records at SNOMED CT granularity and derives ICD categories with a ConceptMap, not the other way round.
In Italy the hospital discharge record is still coded in ICD-9-CM, in the Ministry of Health’s 2007 Italian version, while ISTAT uses ICD-10 for causes of death. The migration of discharge records to ICD-10 has been announced for years and is not yet complete, and the arrival of ICD-11 moves the horizon again.
Implications
In exchange models, vocabularies plug in through three constructs: the CodeSystem (the vocabulary, identified by OID or canonical URI), the ValueSet (a context-appropriate subset of codes, such as discharge diagnoses) and the ConceptMap (the formal mapping between codes of different systems, such as ICD-9-CM to ICD-10). In CDA R2 these references are OIDs inside the code and value elements; in FHIR — HL7’s REST specification, at Standard for Trial Use status on this date — they become first-class resources.
The practical consequence is that mapping costs something. A ConceptMap from SNOMED CT to ICD-10 is almost always many-to-one and by construction loses detail; the reverse direction is ambiguous and should be kept out of automated flows. Anyone designing an electronic health record must decide at what granularity the primary datum is kept, because that decision governs what remains retrievable years later.
Limits
SNOMED CT is neither free nor adoptable without national membership, and its sheer size makes it unusable without curated Reference Sets: handing the whole International Edition to a clinician entering a diagnosis is impractical. LOINC covers the laboratory well but thins out for non-instrumental clinical observations. ICD, however well established, compresses by design and cannot bear the weight of a fine clinical description. On its own none of the three suffices for a real system, and together they require mappings maintained over time — the hidden cost that weighs more than the licence.
https://www.nlm.nih.gov/pubs/techbull/jf17/brief/jf17_snomed_ct_release.html https://www.nlm.nih.gov/healthit/snomedct/index.html https://loinc.org/news/loinc-version-2-59-and-relma-version-6-18-available/ https://www.who.int/classifications/icd/en/ https://www.hl7.org/fhir/ https://www.noze.it/en/insights/snomed-loinc-icd-terminologie/
Cover image: Screenshot of a SNOMED browser showing a defined clinical concept with its hierarchical IS-A relationships and associated attributes — diagram by Steschu, CC BY-SA 3.0 — https://commons.wikimedia.org/wiki/File:SNOMED_defined_concept.jpg